 |
ADVANCED IMAGING CENTER PHYSICIAN NEWS |
June 1, 2000 |
INTERSETING CASE PRESENTATION
State-of-the-art imaging of Acute Brainstem Stroke: MR DIFFUSION
 |
 |
 |
 |
| Fig. 1 | Fig. 2 | Fig. 3 | Fig. 4 |
|
ADVANCED IMAGING CENTER PHYSICIAN NEWS |
June 1, 2000 |
|
|
|
|
| Fig. 1 | Fig. 2 | Fig. 3 | Fig. 4 |
Clinical Presentation: Patient is a 67-year-old female who presented with difficulty walking, tingling/numbness in left side of face and right leg, and vomiting. STAT MRI with Diffusion was performed at AIC to rule out a possible stroke.
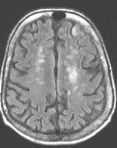
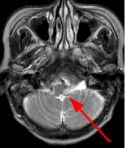
MRI Findings: In the supratentorial regions, some atrophy and chronic small vessel deep white matter ischemic changes were observed (Fig. 1) but no acute lesion or infarct was observed on MR diffusion. In the posterior fossa, however, a subtle small 1 cm hyperintensity can be seen in the left side of medulla on T2 weighted (Fig. 2) and FLAIR images (Fig. 3). This can be seen with an infarct, but its age would remain indeterminate. The MR diffusion image (Fig. 4) shows hyperintensity in the same region consistent with an acute infarct (arrows) as opposed to chronic ischemic changes.
Final Diagnosis: Based on the MR appearance, diagnosis of acute lateral medullary infarct was provided. This is a classic appearance of a posterior inferior cerebellar artery (PICA) infarct (PICA Syndrome), which may have thrombosed.
Q. What are the clinical symptoms associated with lateral medullary infarcts (PICA syndrome)?
Cerebellar dysfunction (injury to spinothalamic tract); loss of ipsilateral facial pain-temperature sensation (injury to spinal tract and nucleus of CN5); loss of contralateral pain-temperature (spinothalamic tract past cross-over); hoarseness and difficulty swallowing (ipsilateral nucleus ambiguous); taste (nucleus solitarius); nystagmus (irritation of vestibular nuclei).
Q. What is MR Diffusion?
MR diffusion imaging is a non-invasive fast MRI technique in which contrast within the image is based on microscopic motion of water. It relies on the fact that molecules routinely undergo random (Brownian) motion. Ultrafast techniques such as Echoplanar Imaging (EPI) are employed, which require fast high-performance gradients.
Q. What are the MR diffusion findings and the time frame in acute stroke?
Conventional imaging may not be able to detect hyperacute strokes or differentiate acute from chronic infarcts. With MR diffusion, detection of acute infarcts is immediate and differentiation from old infarcts is obvious. This is due to its ability to allow discrimination between cytotoxic edema (present in acute infarcts) from vasogenic edema (seen with a variety of other brain lesions including neoplasms), sometimes not possible with conventional MR imaging. Only cytotoxic edema is hyperintense on diffusion-weighted images. Diffusion MR images show abnormal hyperintensity in acute infarcts from minutes to 7-14 days after stroke.*
For more information, please call me personally at (661) 949-8111.
Ray Hashemi, MD, PhD,
Director*Reference: "Diffusion-weighted MR imaging in acute stroke," American Journal of Radiology, Dec. 1999, pp. 1459-1467.