|
ADVANCED IMAGING CENTER PHYSICIAN NEWS |
November 14, 2000 |
INTERESTING CASE PRESENTATION
ENDOMETRIOMA
|
ADVANCED IMAGING CENTER PHYSICIAN NEWS |
November 14, 2000 |
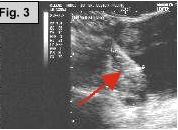
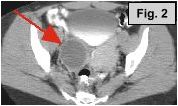
Fig. 1a-c: MRI of the L-spine (sagittal T2 weighted, coronal scout, and coronal MR Myelogram, respectively) demonstrates an incidental 4-5 cm cystic-appearing mass in the right pelvis on limited views of the pelvis. Fig. 2: a helical CT image of the pelvis, revealing a 4x5 cm low-density mass in the right hemipelvis to the right of the uterus. Fig. 3: Pelvic ultrasound shows a moderately enlarged right adnexa measuring 5 cm with low-level echoes.
CLINICAL PRESENTATION: This 38-year-old female presented to the office of Dr. Pamela De Silva with low back pain and falling down the stairs. Patient had a history of an ovarian cyst removed several years ago. On physical exam a mass was felt. Initially, a pelvic ultrasound was obtained at an outside facility revealing no abnormality. Subsequently, an MRI of the lumbar spine was ordered at AIC for evaluation of low back pain. The MRI findings necessitated a helical CT of the abdomen/pelvis and a repeat ultrasound of the pelvis, which were also performed at AIC.
IMAGING FINDINGS: Fig. 1a-c show MRI images of the L-spine (sagittal T2 weighted, coronal scout, and coronal MR Myelogram, respectively). They demonstrate mild scattered disc bulges and an incidental 4-5 cm cystic-appearing mass in the right pelvis on limited views of the pelvis. Incidentally, the MR Myelogram (Fig. 1c) also nicely shows the thecal sac and renal collecting systems. Fig. 2 shows a helical CT image of the pelvis, revealing a 4x5 cm low-density mass in the right hemipelvis to the right of the uterus with CT density of about 20 Hounsfield units on pre- and post-contrast images. A repeat transabdominal and endovaginal pelvic ultrasound with Doppler performed at AIC (Fig. 3) showed a moderately enlarged right adnexa measuring 5 cm with low-level echoes.
DIFFERENTIAL DIAGNOSIS: Based on the CT, MRI, and ultrasound findings, a complex cystic or solid adnexal mass was suspected. Low density on CT and low-level echoes on ultrasound are fairly typical of an endometrioma, which was suggested as a possible diagnosis, although a tumor such as a cystadenoma or cystic teratoma could not be excluded.
PATHOLOGIC DIAGNOSIS: The patient underwent exploratory laparotomy by Dr. William Jack Copeland and a pelvic mass was removed. Pathology revealed an endometrioma.
DISCUSSION: Endometrioma, also known as a chocolate cyst, is made from endometrial tissue that has migrated from the uterus and attached itself to a distant site. Although similar to endometriosis, endometriomas form balloon-like shapes. Every month, the endometrial tissue bleeds a little into the endometrioma, causing it to grow. Over time, the blood turns a dark chocolate-brown color; hence the name "chocolate cyst." MRI is an excellent modality to recognize the presence of different blood products in an endometrioma, thus allowing an intelligent diagnosis.
For more information, you may call me at (661) 949-8111, Dr. De Silva at 948-3899, or Dr. Copeland at 945-4581.
Ray Hashemi, MD, PhD,
Director*Clinical information provided by Lancaster physicians Pamela De Silva, MD (internist) and William Jack Copeland, MD (OB-GYN).